Delayed (optimal) cord clamping
What is delayed (or optimal) cord clamping (DCC)?
The umbilical cord links your placenta to the baby.
In the minutes after your baby has been born, the umbilical cord continues to work.
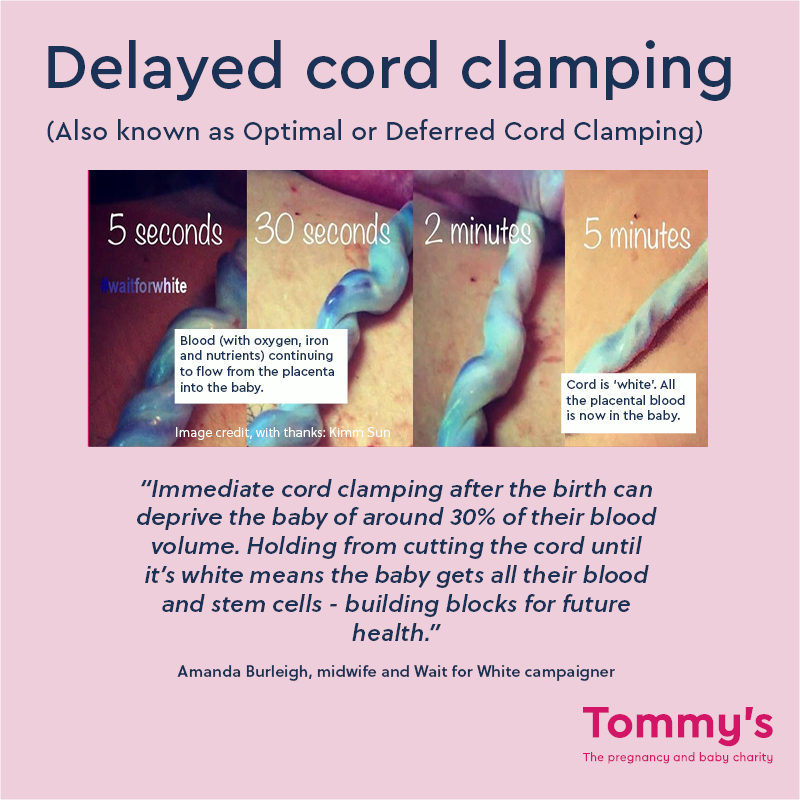
It is still transferring blood, oxygen, and stem cells to your baby while they adjust to being outside the womb and the change from getting their oxygen from breathing instead of through the placenta. .
This blood has many red cells needed to transfer oxygen from the lungs to the heart and brain. It also has many stem cells to repair damaged tissues. Clamping the cord too quickly prevents these from getting to your baby.
It used to be common practice to cut the cord straight after the birth but now guidelines say that delayed (or optimal) cord clamping is better for your baby. This means waiting until the cord has stopped pulsating and has become white before cutting the cord.
The cord should not be clamped earlier than 1 minute after birth.
You can have delayed cord clamping even if you have help to deliver the placenta after giving birth. Find out more about delivering the placenta.
Why is delayed (or optimal) cord clamping important?
The benefits of delayed cord clamping include:
- a full volume of blood in your baby at birth, which gives increased iron levels in the baby up until they are 6 months old, helping with growth and emotional development
- an increased amount of stem cells, which helps with your baby’s growth and helps with their immune system.
There is good research evidence showing that delayed cord clamping can prevent deaths of premature babies as well as improving their overall health prospects.
When is delayed (or optimal) cord clamping not recommended?
Delayed cord clamping is always recommended but your doctor or midwife may need to clamp the cord earlier if there is a health issue that means the baby needs to be treated quickly away from the mother or birthing person. For example, if there are concerns about your baby’s heartbeat or they need breathing support.
Clamping the cord early in this situation is a compromise however as the baby will have less blood in their body.
The ideal care is to provide support with the cord intact. Some units can do this. They have special bedside resuscitation trollies that make it easy to do.
In almost all situations, delayed cord clamping will benefit the baby and will be recommended. But there are some rare circumstances where it may not be suitable, such as:
- if the person giving birth is bleeding heavily and need immediate medical treatment
- if there is an issue with the placenta, such as placental abruption, a low-lying placenta or placenta praevia, vasa praevia
- if the cord is bleeding so the blood is not getting to the baby
- if they baby needs help to breathe (resuscitation). See below for more information on this.
Twins who share the same placenta (monochorionic twins) should not have delayed cord clamping. This is because there is a small risk that blood could move from one twin into the other during the birth.
Find out more about multiple pregnancies.
What if my baby needs help breathing at birth?
Sometimes babies need extra support with breathing when they are born. Midwives and doctors are trained to make decisions to help babies adapt to the outside world.
It may be possible to help your baby without cutting the cord. If they can, your healthcare team will provide any immediate care that your baby needs and keep baby close to you while the cord is intact.
Some hospitals have equipment that gives breathing support without having to cut the cord.
Can I or my birth partner still cut the cord if we have delayed (or optimal) cord clamping?
Yes, you or your birth partner can still cut the cord if you have delayed cord clamping.
Can I have delayed (or optimal) cord clamping with a caesarean section?
You can still have delayed cord clamping if you have a caesarean section, whether it is planned or an emergency. There is no reason why giving birth through c-section in itself would prevent delayed cord clamping.
After the c-section, your healthcare professional will wait to cut the cord (or for your birth partner to cut the cord, if that’s what you want) before cleaning and checking your baby’s health, and passing them to you for a cuddle.
You can talk to the health professionals caring for you about this and have it on your birth plan.
Should I have delayed (or optimal) cord clamping on my birth plan?
Yes. It should be routine in all hospitals but it is helpful to talk to your midwife or doctor about delayed cord clamping during your pregnancy. You can then add your preferences to your birth plan.
If you have a birth partner, talk to them about what you’d like to happen so they are also aware.
Will delayed cord clamping interfere with breastfeeding?
No. The cord is long enough for the baby to be put immediately up to your breast and/or for a skin to skin cuddle, even when the placenta is not yet delivered. Once the placenta is delivered it can be placed beside you and the cord will not prevent any closeness.
What is the difference between delayed (or optimal) cord clamping and milking the cord?
Delayed cord clamping is a natural process where the cord blood is transferred to the baby with no help from health professionals.
'Milking' the cord is when the midwife or doctor gently push the blood through the cord, so it is transferred more quickly. Milking the cord blood is safe to do and benefits the baby as they will get more of the blood, oxygen and stem cells. It usually only happens if there is a rush for some reason. This is usually because the baby needs help with their breathing.
Milking the cord may also be an option for babies born prematurely who are likely to need medical help immediately after the birth. These babies benefit most from getting all the blood from the placenta and umbilical cord and every effort is made to be sure they get it.
Can delayed (or optimal) cord clamping cause increased levels of jaundice in the first week of birth?
There is no increased risk of jaundice in babies who have received deferred cord clamping.
Jaundice is very common in newborn babies and it may happen no matter how soon the cord is clamped after birth.
Your baby will be examined for signs of jaundice within 72 hours of being born as part of their newborn physical examination.
Can I still have delayed (or optimal) cord clamping if I am HIV positive?
You may still be able to have delayed cord clamping if you are HIV positive. Evidence shows that the benefits of delayed cord clamping outweigh the risk of HIV transmission if the mother has been taking antiretroviral medications.
If you are HIV positive, make sure your healthcare team is aware as early as possible in your pregnancy. They can help get the treatment you need to reduce the risk of passing the infection to your baby.
Can I still preserve blood from the cord for medical research?
Umbilical cord blood can be used to treat and cure many life-threatening diseases.
Some parents want their cord blood to be collected at the time of birth and stored so that it is available for medical research.
Banks can still collect high-quality units of cord blood following delayed cord clamping. But it is important that the cord blood is drained as soon as possible following delayed clamping to maximise the potential volume.
Your midwife or hospital maternity unit may have more information about cord blood banking. You can also find out more from the Human Tissue Authority.
Now that delayed cord clamping of at least 1 minute is a routine practice in the UK there is less residual blood in the placenta. However sometimes there is enough blood for donation or for storage in a private cord blood bank.
NICE (2023) Intrapartum care [NG235], National Institute for Health and Care Excellence, London, England Overview | Intrapartum care | Guidance | NICE
World Health Organisation. Optimal timing of cord clamping for the prevention of iron deficiency anaemia in infants. https://www.who.int/elena/titles/full_recommendations/cord_clamping/en/
World Health Organisation (2014) Guideline: Delayed umbilical cord clamping for improved maternal and infant health and nutrition outcomes. Geneva, World Health Organization; 2014 (p.4): http://apps.who.int/iris/bitstream/handle/10665/148793/?sequence=1
Lawton, C. et al. Enhancing endogenous stem cells in the newborn via delayed umbilical cord clamping, Neural regeneration research vol. 10,9 (2015): 1359-62: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4625484/
The American College of Obstetricians. (2020) Delayed Umbilical Cord Clamping After Birth. https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2020/12/delayed-umbilical-cord-clamping-after-birth
Resuscitation Council UK. Newborn resuscitation and support of transition of infants at birth Guidelines. https://www.resus.org.uk/library/2021-resuscitation-guidelines/newborn-resuscitation-and-support-transition-infants-birth
McDonald SJ, Middleton P, Dowswell T, Morris PS. Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes. Cochrane Database of Systematic Reviews 2013, Issue 7. Art. No.: CD004074.
Human Tissue Authority (2020) Key Cord blood banking information https://www.hta.gov.uk/guidance-public/cord-blood-banking/key-cord-blood-banking-information
BAPM (2020) Optimal Cord Management in Preterm Babies: A Quality Improvement Toolkit Optimal Cord Management Toolkit | British Association of Perinatal Medicine (bapm.org)
Review dates
